
by Aaron Jonas Stutz
Something really struck me about an interview that former Reagan Administration budget chief (and remarkably forthright internal critic) David Stockman gave to Yahoo! Finance on Friday. In this interview Stockman claims that the Affordable Care Act–that is, Obamacare–is “the worst law ever passed in the last four decades by the federal government.” Stockman continues, describing it as “a massive entitlement to end all entitlements,” asserting:
It is going to cause a fiscal hemorrhage that is not even yet anticipated. It will tie up one-sixth of GDP in the most monstrous, massive, bureaucratic snarl that you can’t imagine. So therefore this needs to be stopped before it becomes operational.
This is one of those moments where the basic classroom exercise of delineating what is fact and what is opinion is quite necessary and useful.
I am prepared to accept the part about 1/6 of US gross domestic product being encompassed–in the not so distant future–by Medicare, Medicaid, and Federal or state-run exchanges for buying private insurance policies. Currently, private and public healthcare costs are already more than 1/6 of US GDP, which is one of the biggest reasons why making insurance more affordable and providing technology, organization, and education concerning preventive healthcare is in every American resident’s long-term interest. Add to that the growing demographic momentum of Baby Boomers entering the ranks of the aging–and thus, bringing with them more costly long-term healthcare needs–and it should be clear that it’s no simple task to get healthcare technology, product, and service supply to meet growing aggregate and per capita demand. Here, Stockman is reasonably boiling a very complicated phenomenon down to a simple fact. Aggregate healthcare costs in the United States will continue to rise in the coming years, likely taking on an even greater proportion of national GDP.
It’s Stockman’s bit about an unimaginably “monstrous bureaucratic snarl” that cannot reach escape velocity from the category opinion’s gravitational pull. There are some very good reasons to hold the opinion that Stockman’s “bureaucratic snarl” characterization is itself really opinion. Not fact.
But … and this is an important anthropological but … it’s not clear from Stockman’s interview what he intends to convey as fact versus opinion. This is what really struck me by the interview. And this is important, precisely because Obamacare is at the center of such an extraordinarily socially contested issue in the United States. The issue is: Who should or should not be insured to receive healthcare? …And who should pay for it? The rhetorical ambiguity of Stockman’s statements about Obamacare should give us pause. Is an experienced economic policymaker simply informing us? Or is he trying to persuade us? Is he basing his catastrophic prediction on sound, critical consideration of his prior assumptions and information? Or is he subtly signaling that certain prior assumptions really shouldn’t be questioned?
Indeed, an anthropological perspective is useful here. Rhetorical ambiguity is important in human social life. Even compared to other highly social primate species, we have unusually intensive long-term, yet often unpredictable interactions with substantial social networks–the membership, interests, and factions within which may change extensively over our lifetimes. Conflicts of interest–with other people, between your own short-term and long-term needs and goals, between your sense of identity, history, or group allegiance and the possibilities offered by change–are inevitable. It’s useful, perhaps necessary to make ambiguous gestures, to say things that may be interpreted in more than one way. Part of socio-cultural competence involves successfully pleasing or appeasing multiple audiences in our network with the same message. But such learned, unreflected social practices of ambiguous discourse can make it difficult to recognize when we hold internally inconsistent moral values. Stockman’s hyperbolic, alarmist statements about Obamacare got my attention because he is otherwise a highly critical, rather unorthodox free-market conservative notably willing to admit when he is wrong, and yet, his ambiguous opinion-masquerading-as-fact rhetoric betrays an uncritical tacit assumption. The part of the economy incorporating healthcare technologies, goods, and services, Stockman seems to be saying, is not for everyone in society. In fact, it further seems to be assumed that those already in the healthcare economy simply cannot afford to allow the uninsured inside the tent. This is the de facto state of affairs now. Although Obamacare does now prevent private health insurance providers from denying new coverage based on preexisting conditions, many people still cannot afford to buy new insurance without an additional mechanism to make premiums and co-pays affordable. If we cannot figure out a public approach to change the economic rules, roughly 48 million American residents will remain without the means to pay for expensive healthcare procedures. And taking a step back, this roughly 1/6 of the population becomes part of a common symbolically violent cultural narrative. This is a dramatic way of defining society’s very existence by exercising and representing exclusion of a subgroup within society. Needless to say, this symbolically produces a very unequal sense and social distribution of power. The thing is, David Stockman almost certainly doesn’t think–let alone say aloud–that those of us insured Americans on the inside simply can’t afford to subsidize the uninsured, keeping them on the outside. I would expect that Stockman–as Milton-Friedman-style free-market supporter, his renouncing of the Reaganomics he initially supported notwithstanding–is concerned with subsidies and Medicaid expansion possibly disincentivizing poor Americans from working more and paying proper insurance premiums with their own income. And he is still probably worried about regulation and public bureaucracy raising supply-side costs, lowering healthcare provider profit margins, and thus, limiting both competition and investment in potentially lower-cost, innovative private solutions. But the effect of his rhetorical ambiguity is a strikingly emotional one. If you agree that Stockman is stating fact–that is, we simply can’t afford a government solution to expand insurance coverage–then hearing Stockman tell his story in such dramatic terms engages you in a process of mythologically taking an excursion from your everyday world. Opposing Obamacare is a magical way of maintaining the status quo. If you disagree with Stockman, it is quite likely that political rhetoric in favor of Obamacare has analogous mythologized and mythologizing emotional effect. Obamacare promises to remake society in a new, inclusive way. We like stories that help us to decisively resolve conflicts of interest.
Taking Another Step Back: Anthropological Engagement with Contemporary Micro-Mythmaking in Political Discourse
So we all have conflicts of interest, not all of which we are healthfully aware. I think, though, that it’d be salutary if we all worked on that. Anthropologists certainly shouldn’t be excepted. The reason for all of us to work together in reflecting over where our conflicts of interest lie sort of boils down to learning as adults to try to be inclusive when we play and not to take it too hard when we get excluded or forgotten. The challenge, of course, is that the adult version of playground social dynamics may involve symbolically woven, socially inherited myths, rituals, identities, and technologies that can couch exclusion in often violent, maximally moral terms. If it’s not witches, sorcerers, sinners bound to burn in Hell or at least necessary to disown on this Earth, inferior neighboring ethnic groups, or threatening and inferior ethnic, religious/sectarian or racial minorities … then it’s simply lazy welfare cheaters and takers. Exclusion among adults magnifies just the fear of what can go wrong in social discourse and (sometimes literally) makes a Federal case out of it. The social process by which this unfolds inextricably involves the kind of rhetorically ambiguous, emotionally moving micro-mythmaking that Stockman exhibited in his recent Yahoo! Finance interview. Of course, academics–anthropologists included–all too often engage in similar practices, producing “If you’re not with us, you’re against us” intellectual ideological divides: between scientists and researchers in the humanities, between cultural and biological anthropologists, between processual and post-processual archaeologists.
Critical Thinking, Not Dramatic and Symbolically Violent Mythmaking
With the current case of Obamacare, what could be framed as a focus for compromise has definitely become the “If you’re not with us, you’re against us” micro-mythmaking and even ritualized political equivalent of trench warfare. There have been undeniably large logistical difficulties in rolling out state and Federal health insurance exchanges. (Don’t expect to be able to buy health insurance this weekend, at least, on healthcare.gov, although I have to say that it is the cleanest, clearest, best designed healthcare or government website I’ve seen. Compare it, for example, to the dense, busy, characteristically difficult-to-follow irs.gov … As a supporter of basic healthcare as a public good in a society that can, in fact, easily afford it with some political will and moral imagination, the approach that the Federal website is taking is encouraging. But back to the main point.) These initial difficulties notwithstanding, the core of the Affordable Care Act–using a combination of public exchanges, subsidies, and fees (or rather, tax penalties) to get almost all of the roughly 48 million uninsured US residents to afford and purchase health insurance–has faced pretty intense political opposition. This political opposition to Obamacare is what got the Tea Party movement going. It’s why many Republican gubernatorial administrations, such Nathan Deal’s right here in Atlanta, have opposed expanding Medicaid to cover more poor residents. It’s why US Congressional Republicans have refused to vote for continuing Federal government funding, using it as bargaining chip in an effort to stop the current healthcare insurance reform effort outright. And it’s why the government shutdown–now almost exactly a week old–seems likely to continue and bump directly up against the deadline to raise the US Treasury Department’s borrowing limit. So … my point is that with such active, well-funded and well-organized opposition to implementing the core provisions of the Affordable Care Act, it may not be surprising if low morale, limited funding, and–indeed–harassment by Congressional committees led to operation and oversight of insurance exchanges turning into an irretrievable bureaucratic mess in the future. This wouldn’t be due to an intrinsic aspect of government institutions as bureaucratically hopeless, something that Stockman seems to fear. And it wouldn’t be due to the costs we would pay upfront–with our tax dollars going toward premium subventions for poorer residents–in order to value and develop a healthier population, which is a fundamentally ethical infrastructural investment in the first place. It would be due to political maneuvering driven by amplifying cycles of mythmaking and ritual theater reinforcing emotionally intense narratives about creating and recreating the very core of moral society.
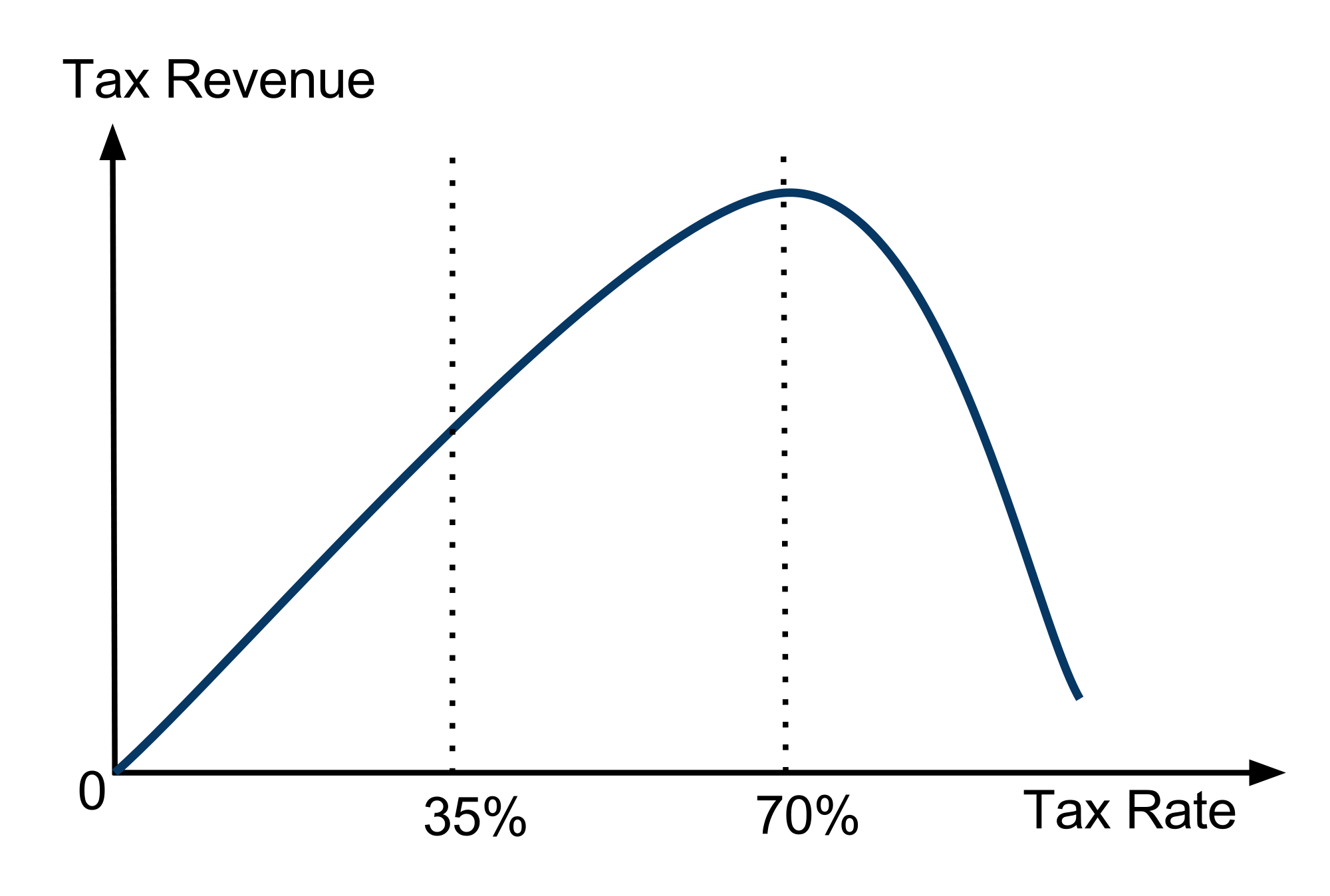
Let’s try to think through an alternative approach, from the starting point of ethically including all residents as deserving access to healthcare. If conservatives were ok with just being worried about marginally but significantly reducing free-loading, increasing the efficiency of government bureaucracy, and reducing the unanticipated costs, they might see the logic that maybe we’re actually to the left of the Laffer Curve maximum, and we actually need to increase tax rates and revenues in order to increase economic productivity, competition, choice, and well-being. Adding new revenues may have short term political costs for Republican national politicians. But it isn’t helpful to cast the story in mythical, cataclysmic terms of a moral battle, especially when there is a political possibility–however idealistic this may sound–for inclusive, deliberative democratic participation and governance that leads to a more sustainable society … and a healthier population constituting it.
References
Trabandt, M., & Uhlig, H. (2009). How Far Are We From The Slippery Slope? The Laffer Curve Revisited (Working Paper No. 15343). National Bureau of Economic Research. Retrieved from http://www.nber.org/papers/w15343
